
 Español
Español
During the present COVID-19 pandemic, most countries in the world have failed at implementing precise measures of testing, contact tracing and quarantining of sick and infectious people. Instead they have implemented the rather crude and desperate strategy of locking everybody up for many weeks.
The latter is obviously not a sustainable strategy, and many countries are beginning to let people out of their homes, knowing full well that the virus is still out there, so opening up will inevitably lead to higher infection rates and more deaths. They just hope to keep severe cases at manageable levels. It is a big balancing act that requires good information in real time, and that is incredibly scarce.
Ideally, we should first let out the people who are least likely to get infected, least likely to infect others, and least likely to die from COVID-19. The idea is to gradually build up herd immunity over the next 12 months with the least number of COVID-19 deaths possible and the lowest collateral damage. That is, we are aiming to minimize total damage from this pandemic.
Who can most safely get out and resume work, education, and leisure activities? The relevant probabilities have three main dimensions: geographic, demographic, and sectoral, and they interact in complicated ways.
In this blog we will provide some empirical evidence to inform strategies to gradually get out of the extremely strict lockdowns in Bolivia.
Geographic variations in risk
Once the virus arrives to a new location, it can have very different impacts depending on a variety of factors. If it arrives to a sparsely populated region with young, healthy, well-informed people practicing good hygiene, the virus will spread slowly, and the vast majority of infected people will likely have either mild symptoms or none at all. But if it hits a densely populated area with malnourished and frail people already suffering from other diseases and without adequate access to water, soap, and sanitation (such as a refugee camp), the impacts could be devastating.
In this section we will present a municipal level analysis of differences in the likely impact of the arrival of SARS-CoV-2 to different municipalities in Bolivia. We considered several dozen potentially relevant indicators from the upcoming Municipal Atlas of the SDGs in Bolivia, and grouped them into the following three broad categories:
- Risk of rapid spread
- Number of main roads entering the municipality
- Centrality of migration (an index reflecting how many other municipalities each municipality is connected with through recent migration)
- Percentage of population living in urban areas
- Percentage of population living in crowded homes (more than 2 persons per room)
- Public transportation intensity
- Underlying health situation
- Obesity level
- Chronic malnutrition level
- Incidence of Dengue, Chagas, Malaria, Tuberculosis and HIV
- Percentage of population older than 60 years
- Response capacity
- Water and sanitation coverage
- Electricity, Phone and Internet coverage
- Share of population who do not speak Spanish
- Education inequality
- Local government budget execution capacity
- Public investment per capita
- Number of doctors per 10,000 inhabitants.
Each variable was converted into an index from 0 to 100, and these indices were aggregated together using weights derived from an online consultation process [1]. The Vulnerability Index reported in this blog uses the 15 indicators that more than 50% of participants agreed had a strong effect on the probability of dying from COVID-19, and equal weights were given to each of them. The 15 indicators chosen were equally distributed between the three groups and they are highlighted in italics in the list above [2].
Table 1 shows the Vulnerability Index for the 339 municipalities of Bolivia ranked from the most vulnerable to the least vulnerable.
Table 1: Vulnerability Index to COVID-19 (based on 15 indicators)
Click on image to expand.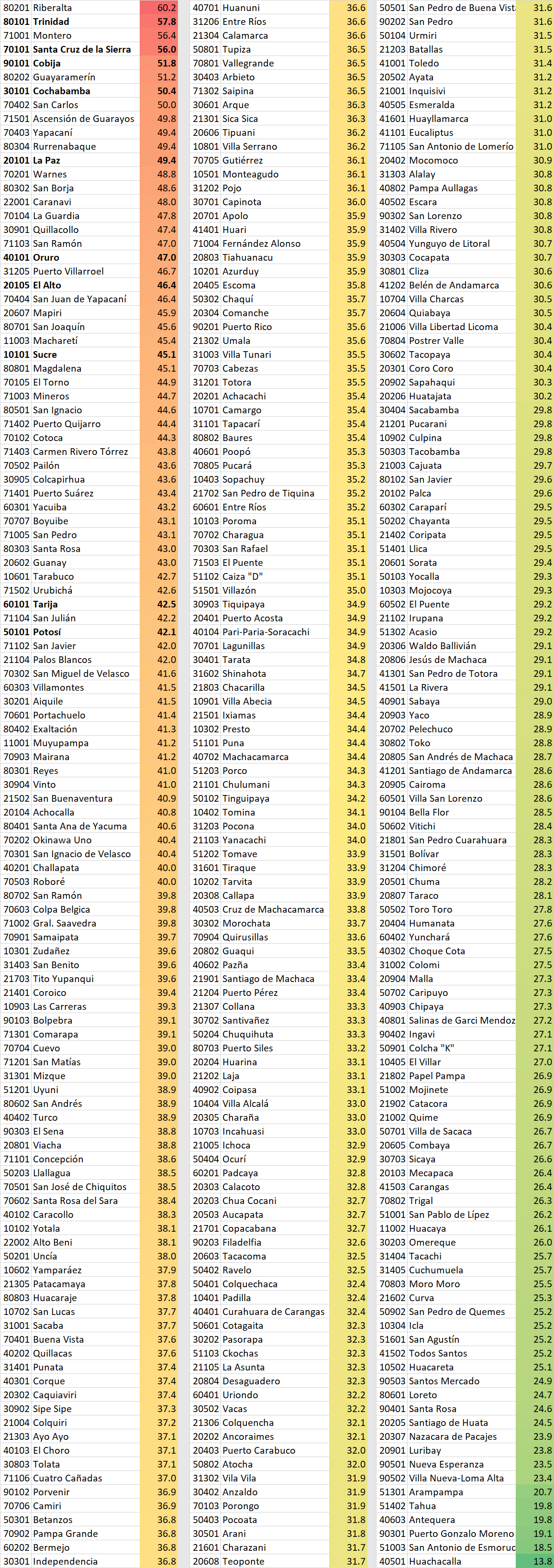 Source: Authors’ elaboration.
Source: Authors’ elaboration.
Note: The 9 state capitals + El Alto are highlighted in bold.
Map 1 shows the spatial distribution of the same Vulnerability Index.
Map 1: Vulnerability Index to COVID-19 (based on 15 indicators)
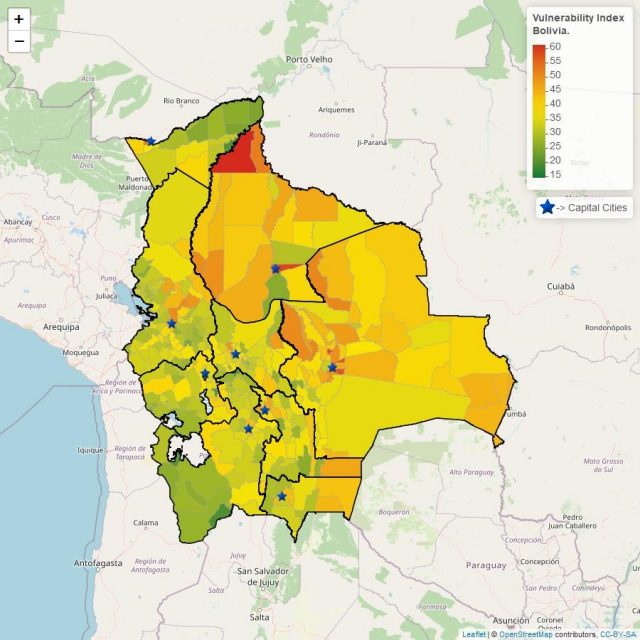
Source: Authors’ elaboration.
Demographic variations in risk
Within each municipality there is considerable variation in risk between different population groups.
It is clear from studies carried out in areas that were infected by SARS-CoV-2 early on that Infection Fatality Rates (IFR) increase exponentially with age and are considerably higher for men than for women [3]. In addition, people with one or more underlying health problems, especially hypertension, obesity, and diabetes, are much more likely to die [4]. Both in the UK and the US, racial differences in IFRs have been observed. Even after controlling for socio-economic and occupational factors, people with darker skin are more likely to die than people with lighter skin [5], possibly due to vitamin D deficiencies that weaken the immune system [6]. This is unlikely to be a significant factor in Bolivia, as long as everybody can get out in the sun every day.
Fortunately, children rarely get seriously ill from COVID-19. Of more than 27 thousand COVID-19 deaths in Italy to date, only 3 were under the age of 18 [7]. There is also some emerging evidence that infected children may not spread the virus as much as adults [8]. Thus, many countries are starting to reopen schools, with increased hand-washing and social distancing efforts, daily disinfection and cleaning of school surfaces, and careful monitoring of the results [9].
Sectoral variations in risk
For people of similar demographic characteristics within the same municipality, risk will vary depending on what kind of activities they carry out. In general, solitary work outdoors is much less risky than working indoors with exposure to lots of different people. Thus, agriculture and construction are relatively safe, while working in a supermarket, a hospital or a dentist office is of high risk [10]. Similarly, solitary outdoor leisure activities, like hiking, golf or tennis, are much safer than indoor team sports like volleyball, basketball or handball. Potentially super-spreading places include night clubs and karaoke bars, among others.
Some high-risk activities are essential and must remain functional even during the strictest lockdowns. In these cases, implementing measures to reduce risk as much as possible is important. Mask wearing in supermarkets, banks, and public transportation is a highly effective way of preventing the virus spread from asymptomatic people to others. Extended opening hours and staggered work schedules reduce crowding and facilitate physical distancing. Switching to online services and home delivery is also possible in many cases. Even many medical services have been successfully transformed and turned into much safer and more convenient telemedicine systems.
Recommendations for loosening the lockdown in Bolivia
A total and uniform lockdown turns out to be inefficient given the large geographic, demographic, and sectoral variations in COVID-19 risk. It is also highly damaging to people’s mental, physical and economic health, and clearly unsustainable.
Given that a vaccine is very unlikely to become available at a global scale until late next year at the earliest [11], and given that we have failed at eradicating the virus even after 50 days of the strictest lockdown that could possibly be enforced in Bolivia, the only remaining option to get through this pandemic is to let the virus burn through most of the population in a controlled fashion over the next 12 to 24 months [12].
If we abandon all precautionary measures, infection rates will skyrocket and we will end up with many more daily deaths than we can physically and psychologically handle. Instead we should continue rational precautionary measures and carry out a gradual reopening, starting with the municipalities, the demographic groups, and the sectors with the lowest risk.
Our recommendations for the immediate future are the following:
- Everywhere, we should maintain the following simple measures to limit the infection rate:
-
- No kissing, hugging or handshaking, except with your closest circle of family members and loved ones;
- No unnecessary gatherings of a lot of people, meaning no sports events, no concerts, no carnivals, no festivals, no graduation events, and no religious gatherings;
- Maintain a 2-metre distance from strangers, interact with as few different people as possible, and wear a mask if you have to be close to them (in supermarkets, public transportation, banks, etc.);
- Avoid touching surfaces that a lot of other people touches, and wash your hands thoroughly after touching a potentially infected surface;
- Work and study from home as much as possible, and limit interactions to as few different people as possible.
- When working from home is not possible, implement flexible working hours and staggered work schedules to reduce peak occupancy in public transportation systems and workplaces.
- Everywhere, outdoor work and leisure activities should be permitted, as long as physical distancing is possible. Indeed, people should be encouraged to get fresh air, sunlight and moderate exercise in order to optimize their immune systems. Masks should not be compulsory when exercising outdoors, because they limit the optimal oxygen intake.
- In the vast majority of municipalities, children can get back to school if adequate hygiene facilities are available. It would be safest if teachers are female, under the age of 60, and generally healthy. Teachers with high risk of a severe COVID-19 reaction (older males with high blood pressure, diabetes, or other risk factors) should not get into contact with children. WHO has guidelines on how to reduce risk in schools [13].
- In the vast majority of municipalities, most shops can reopen, as long as clients can maintain adequate physical distancing. Risks would be lowest if shops are attended by young women. Opening hours should be expanded rather than reduced, in order to reduce crowding.
On the other hand, the most vulnerable municipalities need to prepare for a major impact of COVID-19. In all the variations of our Vulnerability Index, Riberalta jumps out as the most vulnerable municipality in Bolivia. It is a big urban municipality (about 100,000 inhabitants) with lots of connections to other municipalities through recent migration, and it provides health services for many surrounding municipalities in the departments of Beni, La Paz and Pando. However, it has a very low coverage of water and sanitation, and high levels of obesity, malnutrition, Dengue, Malaria, Tuberculosis, and HIV. It is a ticking bomb. But for some reason, the government’s index does not flag it as high risk.
Finally, since this is going to take many months to get through, we should use this opportunity to get universal coverage of electricity, telecommunications, and online services. Now is the time for AGETIC to really push forward with electronic government services.
—
Footnotes:
[1] See recording of webinar held on the 6th of May 2020, and this PDF of the polling results.
[2] We are working on a working paper with much more details and which includes a sensitivity analysis, since there are many possible ways of aggregating the indicators. But the results presented here are highly correlated with the other aggregate indices analyzed.
[3] In Germany, for example, the death rate for men between 50 and 80 years is at least double the death rate for women in the same age group (https://www.statista.com/statistics/1105512/coronavirus-covid-19-deaths-by-gender-germany/). In Italy, Spain, China, Peru and Greece, the gender difference is even more pronounced (https://www.businessinsider.com/men-women-coronavirus-death-rates-by-country-worldwide-health-habits-2020-4)
[4] See, for example, Richardson, S., Hirsch, J. S., Narasimhan, M., et al. (2020). “Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized with COVID-19 in the New York City Area.” JAMA. Published online April 22, 2020. doi:10.1001/jama.2020.6775 ( https://jamanetwork.com/journals/jama/fullarticle/2765184)
[6] https://link.springer.com/article/10.1007/s40520-020-01570-8, https://www.bmj.com/content/356/bmj.i6583, https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3571484
[7] https://www.statista.com/statistics/1105061/coronavirus-deaths-by-region-in-italy/
[8] https://dontforgetthebubbles.com/evidence-summary-paediatric-covid-19-literature/
[9] https://www.sciencemag.org/news/2020/05/should-schools-reopen-kids-role-pandemic-still-mystery
[10] https://www.weforum.org/agenda/2020/04/occupations-highest-covid19-risk/
[11]See this article for a discussion of what it takes to develop, test, produce and distribute a new vaccine: https://unherd.com/2020/04/when-we-get-the-covid-19-vaccine/?tl_inbound=1&tl_groups[0]=18743&tl_period_type=3
[12] See https://www.sdsnbolivia.org/en/english-forty-days-of-quarantine-what-have-we-learned/.
—
* Executive Director, SDSN Bolivia
** Economic Research at Centro Latinoamericano de Políticas Económicas y Sociales – Pontificia
Universidad Católica de Chile – CLAPES-UC.
*** Head of Energy, Environment and Economics at Centro Latinoamericano de Políticas Económicas y
Sociales –Pontificia Universidad Católica de Chile – CLAPES-UC
* SDSN Bolivia.
The viewpoints expressed in the blog are the responsibility of the authors and do not reflect the position of their institutions. These posts are part of the project “Municipal Atlas of the SDGs in Bolivia” that is currently carried out by the Sustainable Development Solutions Network (SDSN) in Bolivia.